

Orthodontic treatment with clear aligners is a quickly growing sector of orthodontic treatment. Both the increase in awareness of esthetics and the increase in orthodontic treatment demand from adults has fueled the demand for a more esthetic orthodontic treatment technique. The public demand for fast and esthetic treatment has been addressed by other dental sectors with approaches such as “instant orthodontics” in which crowns or veneers are used to mask malalignment or with products that claim to use “new techniques” to simply align anterior teeth without addressing other aspects of the occlusion that may need treatment to maintain a healthy dentition. Obviously, these types of approaches raise ethical concerns and the need to educate the public as to the shortfalls of these types of approaches. Fixed appliances have become smaller and more esthetically acceptable with the development of ceramic brackets, but they are still more noticeable than clear aligners. Dozens of companies worldwide now offer some type of clear aligner orthodontic product. While research has been done in the area of clear aligners, much of the early research was focused on trying to discredit the use of aligners as an option for orthodontic treatment except for minor crowding or spacing cases. Even so, there was some research that was done to further improve and progress the clear aligner technique. This is still a rapidly developing area and as a result, much of the literature consists of case reports.
 Introduction
Introduction
Prior to 1998, orthodontic clear aligner treatment was predominantly for very minor tooth movement, usually at the end of orthodontic treatment or to treat minor alignment relapse. In 1998, Align Technology, Inc. introduced Invisalign® to the orthodontic market. It used computerized 3D technology to visualize and move the teeth in a virtual model. This technology along with advances in 3D printing and manufacturing efficiencies allowed aligners to be produced in a large numbers and in a timely fashion.
Initial cases were mild crowding or spacing which progressed to cases that needed expansion and/or classification correction. With these case studies that showed the concept would work, another technique was developing to treat orthodontic patients. This clear aligner technique is continually evolving because of research and development in materials, manufacturing techniques, auxiliaries, and computer programming of tooth movement. The aligners available today are vastly different than those available in 2000. Many different types of aligners are available today throughout the world and marketed to treat everything from mild to more severe malocclusions.
This article will discuss the current techniques used for problems that may arise during treatment with aligners, and for treatment of the more challenging aspects of various malocclusions. The available literature for aligner treatment has grown over the years with several clinical trials being done that examine how well the predicted outcomes compare with the actual outcomes. However, while this is informative data, it is only relevant to the aligner system and materials used and may become dated quickly because of the advance made in various technologies. As a result, most of the literature for current techniques used in clear aligner treatment comes from case studies.
Treatment with clear aligners
Regardless of the aligner system chosen, the practitioner should dictate the treatment plan which results in how the aligner treatment proceeds and where the teeth are to be moved. This is true if aligners are fabricated from a series of models where the teeth have been manually manipulated or from digital models in which the teeth are manipulated by computer or technicians. The following techniques can be used with most aligner systems, unless specifically noted, to treat the following orthodontic problems.
Openbite
As with fixed appliances, anterior openbites can be addressed by either intrusion of posterior teeth to allow the mandible to rotate closed, or by extrusion of the anterior teeth, or a combination of both. It is up to the practitioner to decide the best approach within the framework of treatment objectives and stability.
Extrusion of anterior teeth can be accomplished with attachments. Attachment shape and location have been shown to affect retention of aligners. Hennessy wrote a recent article describing the optimized attachments developed for use with Invisalign® including those for extrusion of anterior teeth which are pre-activated beveled attachments. Even with extrusion of anterior teeth, an advantage of using aligners for treatment is the posterior intrusive affect that the aligners will have on the posterior teeth which also facilitates closure of the anterior openbite. This posterior intrusive affect is beneficial in treating cases with crowding and minimal overbite. With fixed appliances, posterior arch expansion may tip the molars or premolars with equal ease. This tipping results in extrusion of the lingual cusp. In turn, the anterior openbite is made worse. Also with fixed appliances, if crowding is resolved with incisor proclination, the outcome of this tipping is a relative intrusion of the teeth again making the openbite worse. shows a case with crowding and minimal overbite. Aligners were able to control the vertical and maintain the overbite while also resolving the crowding. Unfortunately, the literature contains only anecdotal evidence from case studies. National Dental PBRN is currently conducting a prospective clinical trial to examine anterior openbite treatment success and stability which will fill a void in the literature.

Figure 1 Fig 1 (A) Initial photos of 12 years 2-month-old girl with Class III tendency, moderate upper and lower crowding, and a shallow overbite. (B) Final photos after 16 months of treatment with Invisalign. Aligners provide an intrusive force on the posterior teeth which helps control the vertical dimension. As a result, crowding was resolved without creating an anterior openbite.
Extrusion of anterior teeth with attachments and intrusion of posterior teeth with the aligner could take an extended amount of time depending on the amount necessary or may need either a greater force(particularly for posterior intrusion). In these instances, TADs have been used to facilitate both types of movements.
Deepbite
Deepbites are generally treated by anterior intrusion which can be difficult with aligners. To facilitate this movement, Invisalign® uses attachments on the premolars for anchorage while an active intrusive force is placed on the incisors as well as bite ramps built into the lingual of the aligner of the upper anterior teeth that act as a bite plane. Incisor intrusion can be difficult with aligners or take a protracted amount of time and no data exist on the effectiveness of these auxiliaries. In these instances, intrusion can be facilitated with TADs. Bowman et al show a very nice method to intrude upper incisors by creating a dimpled extrusion of the buccal surface of the aligner with a Hilliard plier (Dentsply Raintree Essix Glenroe, Sarasota, FL) and then cutting a notch. Vertical elastics are then used from the notched aligner to TADs placed in the anterior buccal vestibule to provide the intrusive force.
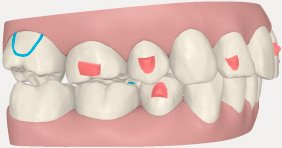
Fig 2. Attachments placed on premolars provide anchorage for the intrusive force place on the upper and lower incisors. If no attachments were placed, the anterior intrusive force would cause the posterior of the aligner to lift off the teeth which would result in little, if any, intrusive force applied.
Space closure
Closure of extraction spaces presents the challenge to finish with parallel roots. While this is true with any appliance, when using fixed appliances, root-tip bends can be placed in archwires as necessary to finish the case. However, aligners present a unique challenge because the goal is to move the teeth with pure translation in order to prevent the tipping from occurring in the first place because a tipped tooth is difficult to correct and can take a prolonged time to upright with aligners alone. As a result, when using aligners, methods to address this issue include aligners in combination with fixed appliances, auxiliaries placed on the tooth to change the point of force application, TADs to eliminate unnecessary forces on anchorage, and attachments to accomplish this movement. The use of aligners and fixed appliances is particularly a good option when a molar needs to be moved mesial to close an extraction space or when roots are long which increases the probability of tipping as shown in Fig. 3. TADS have been used as anchorage to avoid placing forces on teeth that could cause unnecessary tipping as described by Bowman et al.Choi et al.describes a unique method using a segmental aligner for the anterior teeth and using TADs to retract this segment. While no clinical trials have been done, case studies have shown that large attachments placed on the teeth to be moved may help prevent tipping, however, experience tells us that this is highly unpredictable. Samoto and Vlaskalic recently published treatment of an extraction case treated using Invisalign® and used knowledge of the biologic tooth movement cycle to control tooth movement and tipping by sequencing which teeth were moving at any particular time and altering the aligner wear time. Preferably, attachments could be designed to help control the tooth movement or the anchorage segments. Womack and Boyd have demonstrated that vertical or horizontal attachments as shown in Fig. 3A on the molars, premolars, or canines can help, but there is no reported data that shows efficacy, and as shown in Fig. 3B and C this does not always work and can result in molar tipping which is also frequently seen in treatment with fixed appliances as well. Correction of this tipping often requires a period of fixed appliances as shown in Fig. 3D and E. Recently, Invisalign® developed attachments to control posterior anchorage in cases requiring extraction and retraction of anterior teeth. These strategies work by placing a force that creates a moment in the opposite direction to counter the tipping moment (Fig. 4A). Since these are new, little has been reported, but as seen in Fig. 4B and C after 6 months of treatment, the upper posterior anchorage segment appears to be maintaining its original position.
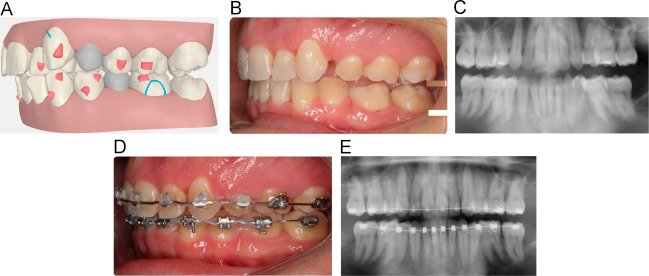
Fig 3 (A) Rectangular attachment was placed on the lower 1st molar as a preventative to crown tipping during mesial movement of the molar needed for correction of the Class II. However, molar tipping may occur as seen in (B) and (C). This can be corrected easily with a period of fixed appliances as seen in (D) and (E).

Fig 4 (A) Attachments on the upper molars and 2nd premolar are pre-activated when placed which creates a clockwise moment to oppose the counter-clockwise moment created when retracting the anterior teeth. (B) The clincheck illustrating where teeth should be after 6 months of treatment which is confirmed in (C).
Crossbites
Difficulty in the correction of crossbites is a factor of location in the mouth and the depth of the bite. Minor anterior or posterior crossbites with a bite depth up to about 10% are usually not difficult to treat with just the usual aligner treatment. Anterior or posterior crossbites with a bite depth greater than approximately 10% usually requires some other considerations to open the vertical to allow the tooth in crossbite to clear the opposing teeth such as anterior bite ramps that are available on the Invisalign® aligners or placing cold-cure acrylic on the occlusal surface of the aligners while the crossbite is being jumped. In order to avoid occlusal trauma to the teeth as the crossbite is correcting, the aligners may need to be worn full-time including while eating until the crossbite is jumped. Crossbite correction of posterior teeth as shown in Fig. 5A may be facilitated by placing attachments on the lingual (Fig. 5B) and/or using crossbite elastics (Fig. 5C) when the movement is programed in the aligners. The result of this type of setup is shown after 3 months in Fig. 5D and E.
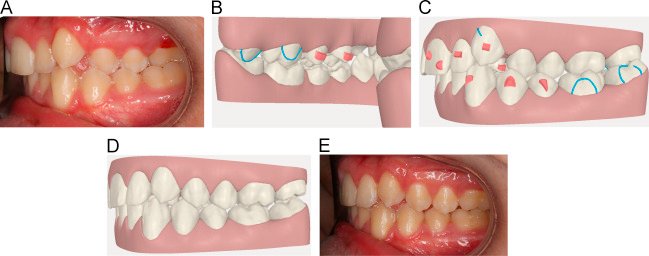
Fig 5 (A) Patient with crossbite of all premolars and molars was treated with lingual attachments on the upper premolars (B) and crossbite elastics from buttons placed on the lingual of the upper molars and buccal of the lower molars (C). Crossbite correction can be seen in a scan after 3 months of treatment (D) and the clinical treatment photo (E).
Extrusion/settling
Often a ClinCheck for Invisalign will require the teeth to extrude into the final desired occlusion. While attachments are automatically placed to facilitate this movement when a threshold of greater than 0.4 mm is reached, movements less than this are expected to occur unaided. Frequently, this does not occur and gingival beveled attachments can manually be placed on the desired teeth in the ClinCheck. As another option, vertical elastics from buttons can also be used to facilitate this movement independent of the magnitude of the movement (Fig. 6).
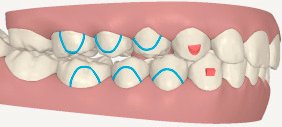
Fig 6 Clincheck showing precision cut-outs where buttons are placed for vertical elastics to help settle the posterior occlusion.
Class II correction
The correction of a Class II malocclusion with aligners can be treated much like as it is done with fixed appliances. While no clinical trials have been done to determine which methods might be the better choice with aligners, treatment options range from distalization of the upper dentition to protraction of the lower dentition or a combination of both. In younger patients, mandibular growth can also help in the correction of the Class II malocclusion. Fischer presented several cases where he used attachments on molars and premolars to sequentially distalize the maxillary dentition to a Class I without the use of Class II elastics. In one of the cases, 2nd molars were extracted to facilitate the distalization. As in space closure, pure translation during distalization can be difficult with aligners or fixed appliances. Often the posterior teeth are tipped back and care must be taken to then distalize the root and prevent the crown from relapsing and tipping forward. This movement can be difficult with aligners due to force necessary to create the moment that will distalize the root. In addition, anchorage for the distalization comes from the anterior teeth and flaring or anterior movement may occur. This is usually controlled by using the lower arch for anchorage with Class II elastics which can then also assist in distalizing the upper dentition as well as protracting the lower dentition. As with space closure, TADs placed either in the buccal or the palate can be used as anchorage to distalize the upper dentition to Class I or to retract the anterior teeth after extraction of upper first premolars. Both the Carriere Distalizer and the Mara appliance have been used to initially create a Class I molar followed by treatment with aligners to finish the case. Arreghini et al described treating a patient with a Runner which is a series of aligners with ramps build on the occlusal surfaces that resemble Twin Block and are meant to advance the mandible and mandibular dentition. This works well in growing children to take advantage of growth in correcting the Class II malocclusion.
Class III
Treatment approach to Class III malocclusions with aligners is similar to those with fixed appliances. Class III elastics and either maintaining dental compensations or creating dental compensations are often done when a Class III malocclusion is treated by orthodontics only. When surgery is a consideration, the case is decompensated prior to surgery. TADs have been used to distalize the lower dentition in an effort to minimize some compensation, but this approach has its limits and may not full correct the Class III malocclusion.
Concluding remarks
Over the last 16 years, clear aligner treatment has developed from a technique of only treating mild crowding or spacing of anterior teeth to a technique that can be used to treat almost any type of orthodontic problem. However to do so, one needs to understand the limitations of the appliance and to be able to think “out of the box” in treatment planning. Aligner materials and attachments will continue to improve which will allow aligners to fit better and for longer periods of time and result in better outcomes. Research into tooth movement and particularly tooth movement mechanics with aligners and the variation in these movements will allow further development of computer algorithms that are used in sequencing aligner tooth movement. Even so, with the amount of variation that is seen in orthodontic treatment, it will always take a knowledgeable practitioner to treatment plan and monitor treatment with aligners.
Source: Science Direct

